PERSPECTIVE: Small Business Owner Does Not Equal Entrepreneur, And That’s Okay
/by Anthony Price My universe was shaken to its foundation, like a building crumbling to the ground under the force of a 9.0 earthquake, after reading Ben Lamm’s guest column in Entrepreneur magazine: “Stop Calling Everyone an Entrepreneur—They Aren’t.”
I thought this was typical Silicon Valley propaganda, from a hotshot in a hoodie and jeans. But after my less-skeptical self emerged, I began to think there was merit to what Ben was espousing. Ben, the founder of several companies and CEO of a startup, believes that the “entrepreneur” label has become as ubiquitous as Nikes on NBA-wannabes. He says that a lot more people are qualified to manage a “Jamba Juice than take companies from inception, through market traction (paying customers), funding, growth and eventual IPO or exit.”
I full-heartedly agree. Ben comes from a world where solving big “hair-on-fire” problems and scaling a business as fast as possible are crucial to owning a market and attracting OPM: Other People’s Money. This business template requires a steady stream of capital to be pumped into the business as fuel, which most businesses don’t have.
The money that your small business burns through is yours, or if you are lucky, your family’s, friend’s or the bank’s. In reality, a startup business has a limited amount of time to build a business with paying customers, or it will fail. Think of Chobani yogurt in your refrigerator—it’s expiration date is a constant reminder that it will not last forever.
The pressure comes from investors. When you play with OPM, investors are the house, they make the rules, and they want to make lots of money (10, 20, or 30x return or more) from a liquidity event (an exit from your business within five to seven years as a result of selling or going public). In Ben’s view, the mission is the domination of an industry from the playbooks of Facebook, Google and Amazon.
Entrepreneurs Take Big Risks
Entrepreneurs view problems from a unique perspective. George Bernard Shaw, the playwright, said, “The reasonable man adapts himself to the world: the unreasonable one persists in trying to adapt the world to himself. Therefore all progress depends on the unreasonable man.” Entrepreneurs are the unreasonable men (and women), risk-takers, but not gamblers. To them, gambling is working at a job they don’t like, with no future for advancement, for a boss who doesn’t value them. Entrepreneurs are confident in their abilities to solve big problems, assemble a team and scale. They are a special group of people who believe in their vision, talent, version of reality and work ethic.
 The biggest differentiator between an entrepreneur and a small-business owner is that the former wants to solve big problems, grow quickly and takes huge risks. Think Facebook, Google, and Tesla. Facebook has over two billion monthly users, and its mission is: “Give people the power to build community and bring the world closer together.” Google is the most visited website on the Internet. Its mission is: “To organize the world’s information and make it universally accessible and useful.” Founded in 2003, Tesla Motor’s mission is: “To accelerate the advent of sustainable transport by bringing compelling mass market electric cars to market as soon as possible.”
The biggest differentiator between an entrepreneur and a small-business owner is that the former wants to solve big problems, grow quickly and takes huge risks. Think Facebook, Google, and Tesla. Facebook has over two billion monthly users, and its mission is: “Give people the power to build community and bring the world closer together.” Google is the most visited website on the Internet. Its mission is: “To organize the world’s information and make it universally accessible and useful.” Founded in 2003, Tesla Motor’s mission is: “To accelerate the advent of sustainable transport by bringing compelling mass market electric cars to market as soon as possible.”
Small and Powerful
A business consists of coordinated activities that deliver value to customers with the intent of generating a profit to its owners. There are twenty-nine million small businesses in the U.S., which represent 99.9 percent of all businesses.
The U.S. Small Business Administration (SBA) defines a small business as having fewer than 500 employees; organized for profit; has a place of business in the U.S.; operates primarily in the U.S.; is independently owned and operated, and is not dominant in its field on a national basis. Michael Gerber, the author of The E-Myth states, “There is a myth in this country—I call it the E-Myth—which says that small businesses are started by entrepreneurs risking capital to make a profit. This is simply not so.”
Most small business owners make the misguided assumption that because they know the technical work of the business, they understand the business that does the technical work. These are two different things, just as being a home baker doesn’t make one competent to run a neighborhood bakery or a corporate chain of bakeries. Small business owner does not equal entrepreneur.
Compare Ben Lamm’s vision of a startup business on steroids with how most small businesses start. Look at your favorite small business. For example, the guy (Jim) who owns the automobile repair garage down the street probably started because he either worked in the family business or got tired of working for someone else. Jim doesn’t have a grand vision to be as ubiquitous as Pep Boys. Sure, he wants to make money, but the love of his craft, freedom from a boss, quality of life, and a sense that he can shape his destiny are all reasons that usually motivate someone to start or buy a business.
Just Do It
Customers determine winners in business. But a decisive factor for your future success comes down to how you answer this question: Will you be an entrepreneur or a small-business owner? Entrepreneurs take big risks to create something new, while small-business owners provide goods and services that the market needs right now. Each has its own value.
Life as a small-business owner is appealing. There’s no disputing its impact on the American psyche. In our winner-take-all society, we need balance between big-risk takers and steady small businesses. Ben states, “Entrepreneurs, at their core, are rare, transformative and risky. They are going to propel the society forward with big leaps of creative disruption. Small-business owners give us a stable base that de-risks the moonshots and protects us from the fallout of failures.” Our economy needs both the entrepreneur and the small-business owner.
To succeed in business, you have to know whether you’re playing as an entrepreneur who is ready to change the game, the industry, the world, or as a small-business owner seeking to make an impact on a smaller scale. If you’re trying to change the game, put on a pair of Shaquille O’Neal’s size 22, because that’s what changing the game feels like. Your choice whether to be an entrepreneur or small-business owner will affect how you start, fund, manage, and grow your business.
Takeaway: Decide what you will be. Choose one.
__________________________________
This is an edited excerpt from Get the Loot and Run: Find Money for Your Business, by Anthony Price of Hartford. Price is founder and CEO of Lootscout, and an entrepreneur, speaker, panelist, and judge for business competitions. A trusted adviser to startups and growing businesses, his expertise is sourcing growth capital for entrepreneurs. This excerpt is published with permission of the author.
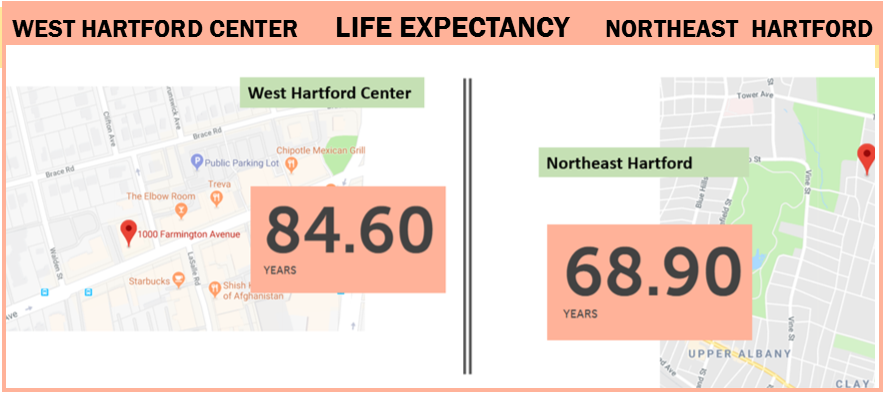 There is variation within cities and towns. In New Haven’s Newhallville neighborhood, life expectancy is 71.7 years. In the neighborhood next door, Prospect Hill, life expectancy is more than a decade longer: 82.3 years.
There is variation within cities and towns. In New Haven’s Newhallville neighborhood, life expectancy is 71.7 years. In the neighborhood next door, Prospect Hill, life expectancy is more than a decade longer: 82.3 years.
 A System of Professional Endorsement is Improving Connecticut’s Workforce
A System of Professional Endorsement is Improving Connecticut’s Workforce
 One of the most common ways lawmakers in marijuana states have attempted to address traffic safety concerns is to establish an impairment threshold for marijuana, a ‘per se’ standard for it, (similar to the 0.08 BAC standards in every state for alcohol).
One of the most common ways lawmakers in marijuana states have attempted to address traffic safety concerns is to establish an impairment threshold for marijuana, a ‘per se’ standard for it, (similar to the 0.08 BAC standards in every state for alcohol). These numbers are high, but they correspond to previous research showing that on any given day, one-third of children consume fast-food… Furthermore, parents’ purchases of fast-food for their children increased significantly during the years examined, with parents reporting increased frequency of visits to most individual fast-food restaurants from 2013 to 2016…
These numbers are high, but they correspond to previous research showing that on any given day, one-third of children consume fast-food… Furthermore, parents’ purchases of fast-food for their children increased significantly during the years examined, with parents reporting increased frequency of visits to most individual fast-food restaurants from 2013 to 2016…
 Unhealthy options, including main dishes, sides, and desserts, remain on kids’ meal menus at most restaurants, and purchases of a kids’ meal plus another menu item for their child have increased. Although future research is required to explain the reasons for these trends, they do indicate that restaurants’ voluntary pledges, as currently implemented, are unlikely to substantially reduce children’s fast-food consumption overall, or increase their selection of available healthier drink and side options.
Unhealthy options, including main dishes, sides, and desserts, remain on kids’ meal menus at most restaurants, and purchases of a kids’ meal plus another menu item for their child have increased. Although future research is required to explain the reasons for these trends, they do indicate that restaurants’ voluntary pledges, as currently implemented, are unlikely to substantially reduce children’s fast-food consumption overall, or increase their selection of available healthier drink and side options.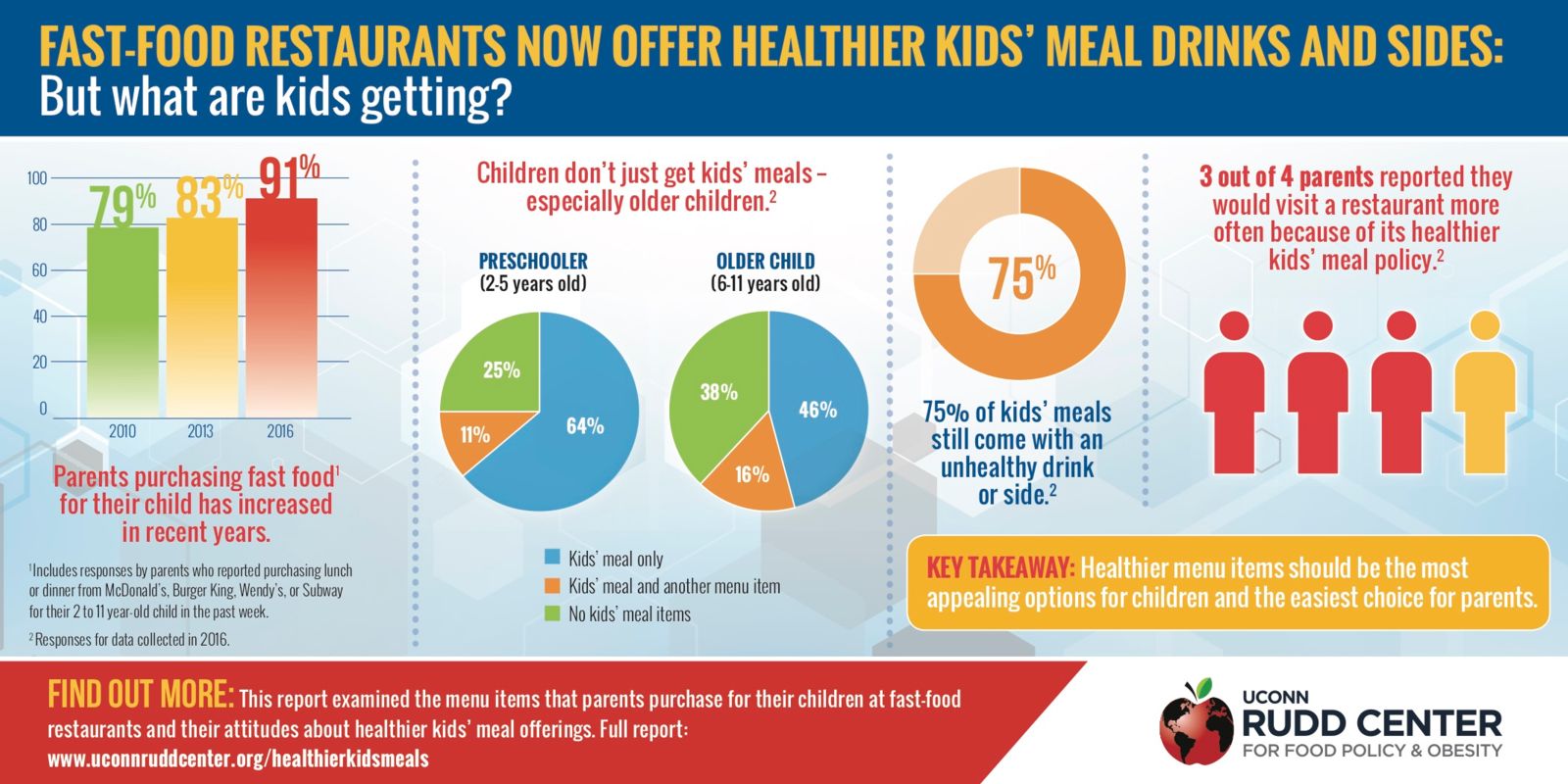
 While we are pleased to see that you share our concerns about the potential impact of Texas v. U.S. on people with pre-existing conditions, as evidenced by your recent introduction of the Ensuring Coverage for Patients with Pre-Existing Conditions Act (S.3388), the safeguards presented in this legislation fall far short of the patient protections encompassed in existing law. This bill as written is far from an adequate replacement for the protections for individuals with pre-existing conditions that are provided under current law.
While we are pleased to see that you share our concerns about the potential impact of Texas v. U.S. on people with pre-existing conditions, as evidenced by your recent introduction of the Ensuring Coverage for Patients with Pre-Existing Conditions Act (S.3388), the safeguards presented in this legislation fall far short of the patient protections encompassed in existing law. This bill as written is far from an adequate replacement for the protections for individuals with pre-existing conditions that are provided under current law.

 Finally, there is the “Stupid Hat Syndrome.” I first heard this expression from a successful businessman, famously generous with both his money and his volunteer board service. He coined the phrase to express his frustration after years of observing “some of the smartest and most successful business people he knew join a nonprofit board and immediately put on their Stupid Hat.” In other words, they habitually checked their immense brain power and experience at the door. The Stupid Hat metaphor may be hard edged, but the phenomenon is real and all too commonplace in the sector. It’s the 800-pound gorilla in the corner, and it’s as true as the truism that in general “you get what you pay for.”
Finally, there is the “Stupid Hat Syndrome.” I first heard this expression from a successful businessman, famously generous with both his money and his volunteer board service. He coined the phrase to express his frustration after years of observing “some of the smartest and most successful business people he knew join a nonprofit board and immediately put on their Stupid Hat.” In other words, they habitually checked their immense brain power and experience at the door. The Stupid Hat metaphor may be hard edged, but the phenomenon is real and all too commonplace in the sector. It’s the 800-pound gorilla in the corner, and it’s as true as the truism that in general “you get what you pay for.” Several years ago, town leaders in Litchfield County implemented a program to share heavy equipment. Ten towns in the area benefit from this program, the Litchfield Hills Public Works Equipment Cooperative, which allows the towns to share major equipment for road maintenance. Two street sweepers and one catch basin cleaner were purchased through the program, which was made possible by a $700,000 grant the council received from the state’s Regional Performance Incentive Program.
Several years ago, town leaders in Litchfield County implemented a program to share heavy equipment. Ten towns in the area benefit from this program, the Litchfield Hills Public Works Equipment Cooperative, which allows the towns to share major equipment for road maintenance. Two street sweepers and one catch basin cleaner were purchased through the program, which was made possible by a $700,000 grant the council received from the state’s Regional Performance Incentive Program. After a lot of hard work in recruitment and creating lesson plans, we had our first meeting in September of 2017. We were both excited and anxious that this day had finally arrived and that our hard work had paid off.
After a lot of hard work in recruitment and creating lesson plans, we had our first meeting in September of 2017. We were both excited and anxious that this day had finally arrived and that our hard work had paid off.
 One student wrote on the before side of the poster that they feared “we might not be able to get along.” However, after our lesson they wrote on the after side of the poster that now they know “we are so similar and can be close friends.” It was truly inspiring to see how much new knowledge they acquired regarding the similarities between the two religions in just one short hour. The kids were so excited to learn this material and fascinated by the common ground.
One student wrote on the before side of the poster that they feared “we might not be able to get along.” However, after our lesson they wrote on the after side of the poster that now they know “we are so similar and can be close friends.” It was truly inspiring to see how much new knowledge they acquired regarding the similarities between the two religions in just one short hour. The kids were so excited to learn this material and fascinated by the common ground.