ConnectiCare, First Health Insurer to Open Retail Store, Adds More
/Holiday shoppers may encounter something new amidst the traditional retail stores vying for attention. Last month, ConnectiCare opened its first storefront location, a 6,000-square-foot standalone building in Manchester. The company plans to open outlets in Bridgeport, Newington and Orange in the coming days, according to David Gordon, ConnectiCare's senior vice president for strategy and product innovation.
"The impetus for taking this step came from listening to our customers," Gordon said. "The key thing that we consistently heard was how they want a choice in how they engage with us." It is a way of “providing face-to-face interactions with our members and our nonmembers, who feel their relationship with us would work better if we were sitting across a table from each other."
ConnectiCare is apparently the first health insurance company in the state to offer services from a retail storefront location. Manchester was chosen after a study of ConnectiCare members, traffic and drive-time patterns and general population figures. The selection of Bridgeport also was based on proximity to significant numbers of ConnectiCare members, and the surrounding population, and are tied to a new partnership with CliniSanitas to offer bilingual facilities for the state's growing Hispanic population.
The flagship Manchester location, near Buckland Hills mall, is staffed by 12 people and includes an area for seminars on various health topics as well as space for yoga and Zumba classes. ConnectiCare's stores in Bridgeport, Newington and Orange will be smaller than the Manchester flagship, which opened in October.
The ConnecticutCare storefronts will be adjacent to CliniSanitas Medical Center locations. The centers will offer primary care, specialty care, urgent care, laboratory and diagnostic imaging, as well as health education and wellness services. All three centers – Bridgeport, Newington and Orange - will offer extended evening and weekend hours, with walk-ins welcome. The centers are to be staffed with medical and administrative staff who are bilingual in English and Spanish.
This expansion is the result of a strategic alliance between GuideWell Sanitas and ConnectiCare to serve the health care needs of Connecticut's growing multicultural population, while helping to address the long-standing disparities in the health status of people from culturally diverse backgrounds, officials said. ConnectiCare is the only health insurance plan being accepted by the CliniSanitas Medical Centers, which will also serve those paying directly for health care services and those with traditional Medicare coverage, the companies recently announced.
CliniSanitas has more than 40 years of health care experience with over 200 facilities in South America. In 2015, the first stateside CliniSanitas centers were opened in Florida. The company explains that their model is focused on improving access to quality primary care services, and delivering the best health outcomes while preventing unnecessary high medical costs, encouraging longer appointments aimed at strengthening the doctor-patient relationship.
CliniSanitas Medi cal Centers is a joint venture between two leading health care organizations – GuideWell Mutual Holding Company and Organización Sanitas Internacional. GuideWell is a U.S.-based not-for-profit mutual holding company and the parent to a family of forward-thinking companies focused on transforming healthcare.
cal Centers is a joint venture between two leading health care organizations – GuideWell Mutual Holding Company and Organización Sanitas Internacional. GuideWell is a U.S.-based not-for-profit mutual holding company and the parent to a family of forward-thinking companies focused on transforming healthcare.
"We're excited to start our journey in Connecticut in partnership with ConnectiCare and GuideWell to bring our proven model of patient-centered care to the diverse community of Connecticut. These new medical centers will build on our successful centers in Miami, Florida, and our experience transforming healthcare in South America," said Dr. Fernando Fonseca, Chief Executive Officer of CliniSanitas.
"The CliniSanitas Medical Centers will help us deliver on our brand promise to make it easy for our members to get the care they need. ConnectiCare is pleased to help bring the people of Connecticut access to the high quality and culturally relevant health care provided by the CliniSanitas Medical Centers," said Michael Wise, ConnectiCare's President and Chief Executive Officer.
A local company for 35 years, ConnectiCare, a subsidiary of Emblem Health, has a full range of products and services for businesses, municipalities, individuals and those who are Medicare-eligible. In September, ConnectiCare, the single-largest insurer on the state’s health exchange, announced it would participate in the exchange in 2017.


 The findings included in this report “provide policymakers, health professionals, public health advocates, industry representatives, and parents an opportunity to address misinformation conveyed through marketing of baby and toddler food and drinks.”
The findings included in this report “provide policymakers, health professionals, public health advocates, industry representatives, and parents an opportunity to address misinformation conveyed through marketing of baby and toddler food and drinks.”


 Reading: children who had no regular early care and education arrangements the year before kindergarten and those whose primary arrangements were home-based relative care or non-relative care tended to score lower than children who were primarily in center-based care or who spent the same amount of time in multiple care arrangements.
Reading: children who had no regular early care and education arrangements the year before kindergarten and those whose primary arrangements were home-based relative care or non-relative care tended to score lower than children who were primarily in center-based care or who spent the same amount of time in multiple care arrangements.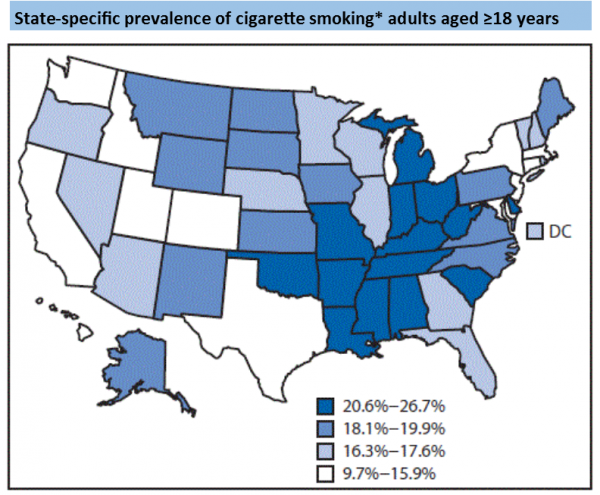
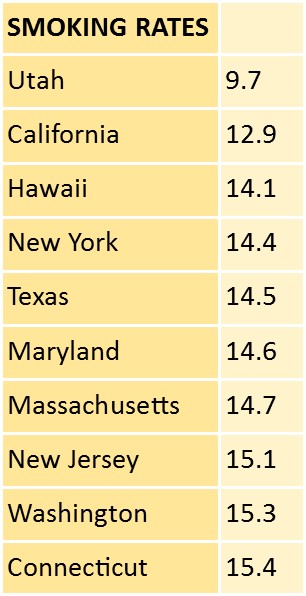 Prevalence of any cigarette and/or smokeless tobacco use ranged from 11.3% (Utah) to 32.2% (West Virginia). Connecticut was 15.3 percent.
Prevalence of any cigarette and/or smokeless tobacco use ranged from 11.3% (Utah) to 32.2% (West Virginia). Connecticut was 15.3 percent.

 According to the most recent data, adult obesity rates now exceed 35 percent in four states, 30 percent in 25 states and are above 20 percent in all states. Louisiana has the highest adult obesity rate at 36.2 percent and Colorado has the lowest at 20.2 percent.
According to the most recent data, adult obesity rates now exceed 35 percent in four states, 30 percent in 25 states and are above 20 percent in all states. Louisiana has the highest adult obesity rate at 36.2 percent and Colorado has the lowest at 20.2 percent.


 At #296 is Glastonbury-based Fiondella Milone & LaSaracina. FML was founded in 2002 “for the purpose of providing professional auditing, tax and business consulting services to a wide range of clients and industries throughout the Northeast,” the company’s website indicates. After working together at Ernst & Young, the firm’s founding partners, Jeff Fiondella, Frank Milone and Lisa LaSaracina launched FML.
At #296 is Glastonbury-based Fiondella Milone & LaSaracina. FML was founded in 2002 “for the purpose of providing professional auditing, tax and business consulting services to a wide range of clients and industries throughout the Northeast,” the company’s website indicates. After working together at Ernst & Young, the firm’s founding partners, Jeff Fiondella, Frank Milone and Lisa LaSaracina launched FML. counting newsletter and the award-winning National Benchmarking Report.
counting newsletter and the award-winning National Benchmarking Report.