Obscured in recent months by the intense presidential campaign, the furor over the price of pharmaceutical company Mylan’s life-saving EpiPen may be moving back to center stage in Washington as questions continue about Connecticut’s policy and the varying impact on school districts across the state. The EpiPen is the widely used medical device that quickly administers a dose of epinephrine to counter allergic reactions.
The cost of EpiPens to Connecticut schools - which keep EpiPens in their nurses’ offices in case a student has a severe allergic reaction - may be defrayed or eliminated by Mylan’s “EpiPens4Schools” program, which gives some schools two twin packs of the medical devices for free. But that is not uniformly true, according to a recent survey by CT by the Numbers, and questions are being raised about the program’s future. 
A report by Connecticut’s Office of Legislative Research found that “over the last decade, Mylan has continuously increased the EpiPen’s cost, from approximately $60 in 2007 to over $600 in 2016 for a pack of two pens. The device requires a prescription and must be replaced annually.”
North Haven, which has participated in the free program, warns that “if the free program is discontinued, it will be a significant financial burden” for the school district. “To satisfy the Connecticut mandate, we must stock one box each of EpiPen Jr. and EpiPen Sr., bringing the total cost to $1,600 x 7 schools = $11,200/year!!!”
In Chaplin, officials have also been using the free program, but note “we will not always be eligible year-to-year,” anticipating “the cost increasing by at least $300 or greater per school.”
Now, the chairman of the U.S. Senate Judiciary Committee says he is considering a subpoena or another method of compelling testimony from Mylan and federal officials, the Associated Press is reporting. Mylan says it agreed to pay $465 million to settle allegations it overbilled Medicaid for EpiPen, but Sen. Charles Grassley says the Justice Department has said there is no "executed settlement." At issue is whether the product should have been classified as generic.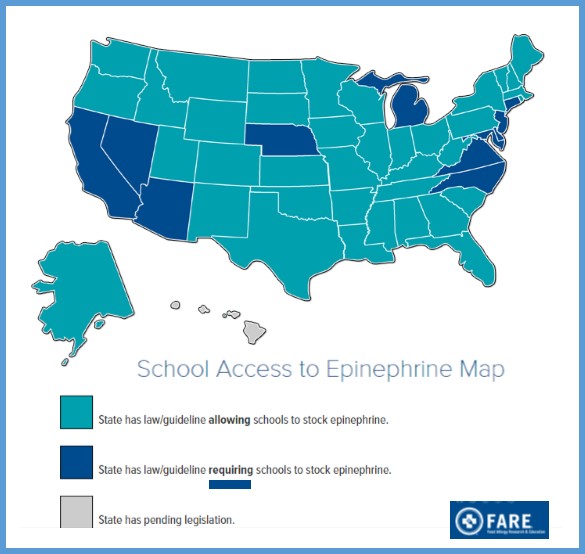
Published reports indicate that Mylan acquired the decades-old product in 2007, when pharmacies paid less than $100 for a two-pen set, and has since been steadily raising the wholesale price. In 2009, a pharmacy paid $103.50 for a set. By July 2013 the price was up to $264.50, and it rose 75 percent to $461 by May 2015. This past May the price spiked again to $608.61, according to data provided by Elsevier Clinical Solutions’ Gold Standard Drug Database.
At a December 1 health forum sponsored by Forbes, Mylan CEO Heather Bresch said “We absolutely raised the price and take full responsibility for that, ” insisting that Mylan’s price increases were justified by improvements the company made on the product.
As the increases were being imposed, Mylan intensified efforts to have states require that EpiPens be made available in schools. Connecticut was among 11 states which passed such a law. The Connecticut General Assembly approved a bill in June 2014 that required all state primary and secondary schools to carry a supply of EpiPens. The new law also allowed school personnel other than a school nurse – if they were properly trained – to administer the epinephrine. Published reports indicate that other states have approved laws allowing student to bring the dispensers with them to classes or encouraging schools to stock the drug.
The Connecticut Department of Education said it does not know how much the new mandate cost the state’s more than 1,300 primary and secondary schools, because the drug is purchased at the local level at a number of approved pharmacies throughout the state, officials told CT Mirror earlier this year.
A number of districts indicated to CT by the Numbers that they had EpiPens on hand in their schools even before passage of the state requirement, and at least one that had participated in the free program previously did not do so this year.
In Eastford, officials purchased one .15 mg dose and one .30 mg dose EpiPen in each of the past three years. The costs increased steadily, from $599.90 in 2021-13 to $740 in 2015-16. In the Region 9 (Easton, Redding) school district, for example, officials indicated that they paid $325 each for three EpiPen twin-packs for the Helen Keller Middle School this year.
Northwestern Regional School District 7 and Regional School District 12, both participants in the free program, have not incurred any costs for EpiPens in recent years. Bolton school officials report that costs have increased in recent years, to approximately $600 per package of two” for a total of $1800 for the year. Region 16 reports that they budget for EpiPen purchases each year, in case the free program is no longer available to them. As of last year, they indicated, the twin-pack price was $535, but they were able to benefit from the company’s free program.
In Cromwell, schools have received 2 twin-packs per school through the free program for the past three years; previously they were purchased by the school district, officials said. In Ansonia, some were provided at no cost, others were purchased. The last time that North Haven paid for the EpiPens was in 2012, when the cost was about $190 each.
 In 2015 the legislature considered, but did not pass, a bill requiring the insurance commissioner to study and report on health insurance coverage of and out-of-pocket expenses for EpiPens, according to the OLR report. The 2014 legislation requires (a) schools to designate and train nonmedical staff to administer EpiPens to students having allergic reactions who were not previously known to have serious allergies and (b) the public health and education departments to jointly develop an annual training program for emergency EpiPen administration.
In 2015 the legislature considered, but did not pass, a bill requiring the insurance commissioner to study and report on health insurance coverage of and out-of-pocket expenses for EpiPens, according to the OLR report. The 2014 legislation requires (a) schools to designate and train nonmedical staff to administer EpiPens to students having allergic reactions who were not previously known to have serious allergies and (b) the public health and education departments to jointly develop an annual training program for emergency EpiPen administration.
The website STAT, which focuses on health and medicine, reports that Mylan Pharmaceuticals has been selling the devices to schools at a discounted price for years, giving them a break from rising costs. But the program also prohibited schools from buying competitors’ devices — a provision that experts say may have violated antitrust law.
Mylan’s “EpiPen4Schools” program, begun in August 2012, offers free or discounted EpiPens to schools. Over 65,000 schools receive free EpiPens through the program; an unknown number of schools buy the epinephrine auto-injectors at a discount. Laws in at least 11 states require schools to stock epinephrine, and keeping a stockpile is incentivized by federal law across the country.
As of last year, the EpiPen4Schools discounted price was $112.10, according to company documents reported by STAT, although the prices cited by Connecticut districts vary.


 explains. “Anyone can become a victim of abuse, but vulnerable older Americans — especially those who are women, have disabilities and rely on others for care or other type of assistance — are among the easiest targets for such misconduct.”
explains. “Anyone can become a victim of abuse, but vulnerable older Americans — especially those who are women, have disabilities and rely on others for care or other type of assistance — are among the easiest targets for such misconduct.”
 As of June 28, 2016, there were 2,007 bakery-cafes in 46 states and in Ontario, Canada operating under the Panera Bread, Saint Louis Bread Co. or Paradise Bakery & Cafe names. Published reports indicate the company has 97,000 employees nationwide and saw a 3.4 percent growth in sales in its third quarter this year. In 2015, it reportedly generated roughly $2.7 billion in revenue. Founder and CEO Ron Shaich
As of June 28, 2016, there were 2,007 bakery-cafes in 46 states and in Ontario, Canada operating under the Panera Bread, Saint Louis Bread Co. or Paradise Bakery & Cafe names. Published reports indicate the company has 97,000 employees nationwide and saw a 3.4 percent growth in sales in its third quarter this year. In 2015, it reportedly generated roughly $2.7 billion in revenue. Founder and CEO Ron Shaich 


 cal Centers is a joint venture between two leading health care organizations – GuideWell Mutual Holding Company and Organización Sanitas Internacional. GuideWell is a U.S.-based not-for-profit mutual holding company and the parent to a family of forward-thinking companies focused on transforming healthcare.
cal Centers is a joint venture between two leading health care organizations – GuideWell Mutual Holding Company and Organización Sanitas Internacional. GuideWell is a U.S.-based not-for-profit mutual holding company and the parent to a family of forward-thinking companies focused on transforming healthcare.
 The findings included in this report “provide policymakers, health professionals, public health advocates, industry representatives, and parents an opportunity to address misinformation conveyed through marketing of baby and toddler food and drinks.”
The findings included in this report “provide policymakers, health professionals, public health advocates, industry representatives, and parents an opportunity to address misinformation conveyed through marketing of baby and toddler food and drinks.” Connecticut's favorite Halloween candy is Almond Joy, with 2,619 pounds of it, on average, ordered each year, the website indicated. Milky Way is Connecticut's second favorite Halloween candy, with 1,366 pounds ordered. M&M's placed third, at 910 pounds on average.
Connecticut's favorite Halloween candy is Almond Joy, with 2,619 pounds of it, on average, ordered each year, the website indicated. Milky Way is Connecticut's second favorite Halloween candy, with 1,366 pounds ordered. M&M's placed third, at 910 pounds on average.


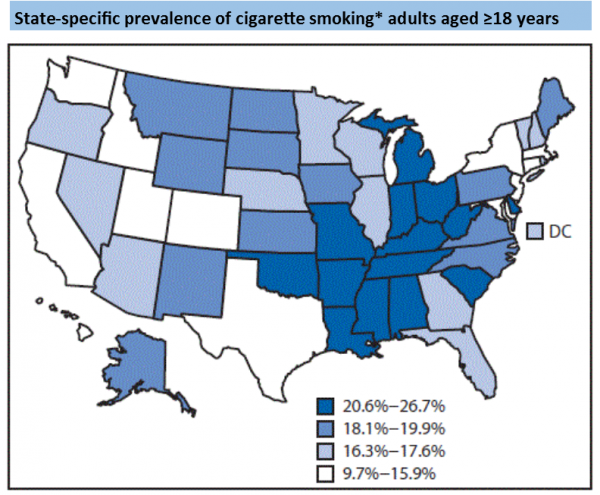
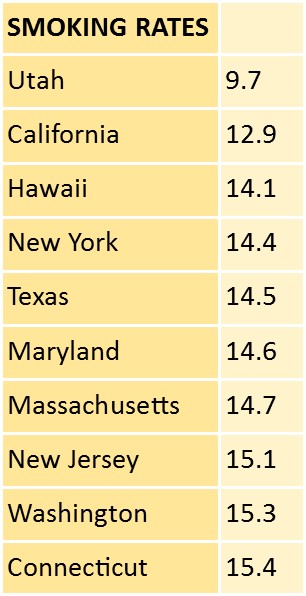 Prevalence of any cigarette and/or smokeless tobacco use ranged from 11.3% (Utah) to 32.2% (West Virginia). Connecticut was 15.3 percent.
Prevalence of any cigarette and/or smokeless tobacco use ranged from 11.3% (Utah) to 32.2% (West Virginia). Connecticut was 15.3 percent.

 According to the most recent data, adult obesity rates now exceed 35 percent in four states, 30 percent in 25 states and are above 20 percent in all states. Louisiana has the highest adult obesity rate at 36.2 percent and Colorado has the lowest at 20.2 percent.
According to the most recent data, adult obesity rates now exceed 35 percent in four states, 30 percent in 25 states and are above 20 percent in all states. Louisiana has the highest adult obesity rate at 36.2 percent and Colorado has the lowest at 20.2 percent.


























{kind=link}